
A Patient’s Guide to Flexor Tendon Injuries and Lacerations (Flexor Digitorum Profundus, Flexor Digitorum Superficialis or Sublimis, and Flexor Pollicis Longus)
Introduction
A deep cut on the palm side of your fingers, hand, wrist, or forearm can damage your flexor tendons, (often called by laymen “leaders”) which are the tissues that help control movement in your hand. A flexor tendon injury can make it impossible to bend your fingers or thumb.
Anatomy
Tendons are tissues that connect muscles to bone. When muscles contract, tendons pull on bones. This causes parts of the body (such as a finger) to move.
The muscles that move the fingers and thumb are in the forearm. Long tendons extend from these muscles through the wrist and attach to the small bones of the fingers and thumb.
The tendons on the bottom/palm side bend the fingers. These are known as the flexor tendons.
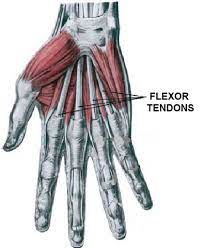
Flexor tendons allow the finger and thumb joints to bend—laceration of the tendons of the ring finger produces the image below:

When you bend or straighten your finger, the flexor tendons slide through snug tunnels, called tendon sheaths, that keep the tendons in place next to the bones. These pulleys prevent bowstringing of the flexor tendons and improve the mechanical efficiency of the system.
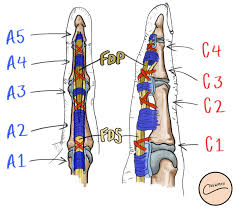
Annular and cruciate pulleys of the finger from a frontal view left and sagittal view right.
Lacerations which occur within the pulley sheath are typically more difficult to repair and have a poorer prognosis (especially Zone 2). Historically, tendon lacerations in this area were treated with delayed grafting, however modern hand surgery typically attempts direct repair within the sheath—and preservation of pulleys as able.

Figure A: Zones of tendon injury in the fingers and thumb—Zone II is associated with increased difficulty and poorer outcomes.
Figure B: Brunner incisions utilized to surgically approach laceration.
Diagnosis
Symptoms
A torn or cut tendon in the forearm, at the wrist, in the palm, or along the finger will make it impossible to bend one or more joints in a finger.
Because flexor tendons are close to the surface of the skin, a deep cut will most likely hit a flexor tendon. In these cases, the tendon is often cut into two pieces.
Like a rubber band, tendons are under tension as they connect the muscle to the bone. If a tendon is torn or cut, the ends of the tendon will pull far apart, making it impossible for the tendon to heal on its own.
Because the nerves to the fingers are also remarkably close to the tendons, a cut may damage them, as well. This will result in numbness on one or both sides of the finger. If blood vessels are also cut, the finger may have no blood supply. This requires immediate surgery.
An uncommon event may occur in sports. Grasping an opponent’s jersey may avulse the flexor tendon from its insertion. The finger may not move properly after the episode is associated with the name “jersey finger.”
Occasionally, flexor tendons may be partially cut or torn. With a partial tendon tear, it may still be possible to bend your finger, but not completely. These types of tears can be difficult to diagnose.
Hand Surgery Examination
The most common signs of a flexor tendon injury include:
- An open injury, such as a cut, on the palm side of your hand, often where the skin folds as the finger bends
- An inability to bend one or more joints of your finger.
- Pain when your finger is bent.
- Tenderness along your finger on the palm side of your hand
- Numbness in your fingertip
The hand surgeon then examines the hand to determine its vascular status and neurological status. The surgeon will also typically test the ability of the finger to flex at each joint.

Testing the sublimus/superficialis tendon left image and Profundus tendon right image.
Surgical Treatment
Almost all flexor tendon injuries require surgery (some partial lacerations less than 50% may be treated without surgery). Surgical timing depends upon the injury. If the finger has been injured and has ischemia from laceration of both digital arteries—typically expedited repair and exploration are indicated. For the isolated flexor tendon injury with a perfused finger (even with digital nerve laceration) repair within the first two weeks after injury is within the standard of care. Surgery if elective can be performed as an outpatient, utilizing a regional anesthesia. A general anesthetic is typically not necessary.
Special incisions are utilized to identify the laceration and find the two ends of the tendon. The incisions are designed not to cross a flexion crease at a right angle. The most common incision is called a Brunner, but midaxial incisions may also be utilized. The incisions can look scary initially, but typically heal with good cosmesis.
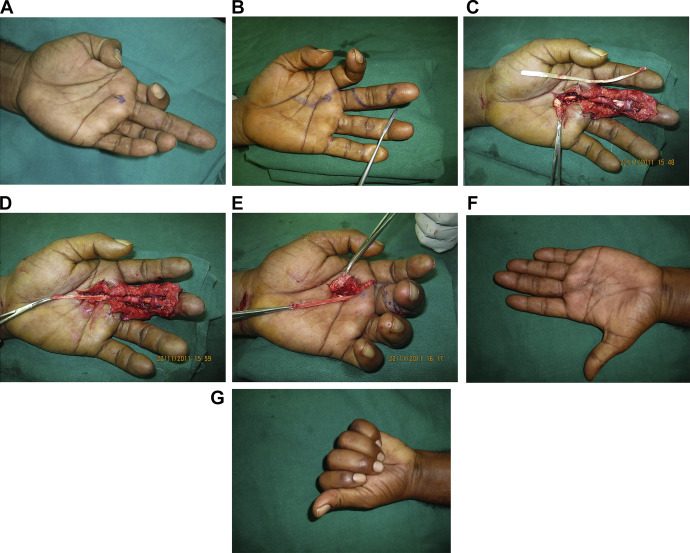
Sequence of surgical repair images for laceration of both tendons of left long finger:
A) Inability to bend finger
B)Planned surgical incision
C) Surgical incisions Brunner of finger
D/E) Surgical exposure and repair
F) Note final good cosmesis and healing of incision
G) Function after repair—note improved function, but not full function.
Recovery from Surgery
Patients are typically placed into a plaster splint which is not removable for 1-2 weeks after surgery with the fingers and wrist bent. Hand therapy and application of a plastic splint are begun between 1-2 weeks after surgery. Hand therapy is a key component to improving outcomes from tendon surgery. Hand therapy may be required 3-5 times per week for up to four months.

A dorsal blocking splint for flexor tendon injuries
It can take up to 3 months before the repair heals and your hand is strong enough to use without protection. It may take another month or so before your hand can be used with any force.
Over the last several decades, advanced research and experience in the treatment of flexor tendon injuries have resulted in improved patient outcomes. Flexor tendon injuries, however, can be challenging to treat.
Despite extensive therapy, some patients have long-term stiffness after flexor tendon injuries. Sometimes, a second surgery is required to free up scar tissue and to help the patient regain motion. Unfortunately, stiffness, tendon rupture and impaired function may all accompany long term results of flexor tendon injury.

